
A Potentially Revolutionary Year for the Wet AMD Market
Will implants from Ocular Therapeutix and Eyepoint become the new Standard of Care for wet AMD?

Implants from Ocular Therapeutix and Eyepoint may become the new standard of care for patients with wet AMD. This article will focus on Ocular’s upcoming Sol-1 readout in February or March.
Background
First, I want to acknowledge that many others have done great work looking at these companies, including, but not limited to, BalaBio (Substack and X) and @houndcl on X. Please check out their write-ups on the subject as well.
Wet Age-Related Macular Degeneration (AMD) is a large global market, characterized by the remarkable success of anti-VEGF therapies. In 2024, the global market for anti-VEGF therapies exceeded $15B.
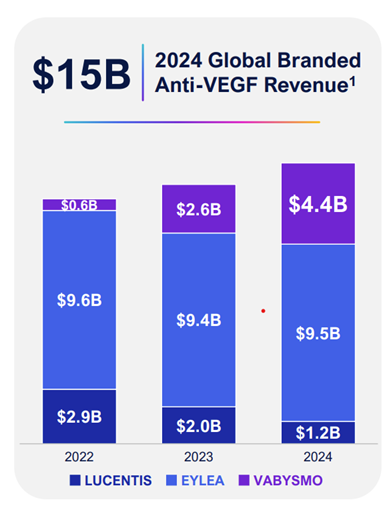
Source: Ocular Therapeutix Investor Presentation
A Medicare claims-related study found the prevalence of wet AMD in patients aged 65 and above to be roughly 1.2-1.3%. Therefore, as the baby boomer generation ages, the market is likely to continue to grow. (https://pmc.ncbi.nlm.nih.gov/articles/PMC11695844/)
Pathophysiology
Age-related macular degeneration (AMD) can be divided into two subtypes: wet AMD and dry AMD. Typically, dry AMD precedes wet AMD. Dry AMD is characterized by the buildup of drusen (lipid/protein deposits). Wet AMD, or neovascular age-related macular degeneration, is a chronic retinal disease where abnormal choroidal blood vessels (CNV) grow under/within the macula and leak fluid/blood, damaging vision. The late stage of AMD is referred to as geographic atrophy (GA), characterized by patches of dead retinal cells.
To give a bit of background on the anatomy of the eye, there are two types of photoreceptors in the eye, rods and cones. They both feed into ganglion cells to the optic nerve, which transmits the electrical signal from the eye to the brain. Rods are 100-1,000x more light-sensitive than cones but only support black-and-white vision. They are great for night vision, peripheral vision, and sensing movement. Many rods converge onto a single downstream neuron, which enables excellent sensitivity but poor resolution. Cones are the “HD” part of vision. They enable color vision and give detailed, sharp pictures. Cones dominate in the fovea, whereas rods dominate outside the parafovea/perifovea.

The center of the macula is called the fovea, as shown in the diagram above. AMD is a disease of the macula, so it primarily affects cone cells.
The primary etiology of dry AMD lies in a dysfunctional Bruch’s membrane. The retinal pigment epithelium (RPE) constantly exports lipoprotein-like particles towards Bruch’s membrane. As people age, Bruch’s membrane thickens, crosslinks, and calcifies, reducing permeability. As a result, these lipoprotein waste products accumulate between the RPE and Bruch’s membrane. This is called drusen. At this point, a cascade of events leads to vision loss. First, there is increased oxidative and mitochondrial stress due to reduced nutrient flow in and waste out. This further impairs import and export and leads to increased drusen formation. Second, complement components in drusen create a chronic microinflammatory environment. Eventually, this leads to cone cell death and vision loss.
Dry AMD can convert to wet AMD when abnormal blood vessels breach Bruch’s membrane and grow towards or into the retina. The dysfunctional accumulation of drusen at Bruch’s membrane creates an environment that upregulates VEGF and other angiogenic signals, bringing blood flow to the area to remove waste and restore nutrient flow. These blood vessels leak fluid, lipids, and blood, leading to retinal swelling and rapid distortion of central vision. Wet AMD is classified into three stages based on how far the abnormal blood vessels have penetrated the retina.
· Type 1 CNV (sub-RPE) – beneath the RPE
· Type 2 CNV (subretinal) – between RPE and photoreceptors
· Type 3 (RAP) – intraretinal neovascularization with choroidal involvement
Disease Symptoms and Features
Dry AMD:
There are often no symptoms in the early stage of dry AMD. In the intermediate stage, there is slightly blurred central vision, trouble in dim light, and slower reading. In late stage or GA, there are missing spots in the central vision, difficulty recognizing faces or reading, and glare issues. However, peripheral vision is typically preserved.
The prognosis of dry AMD before GA is positive. Lifestyle factors and supplements can reduce the risk of progression. Once GA is present, cells have died, so there is no restoring vision. Further vision loss can be reduced with treatment.
Wet AMD:
Common symptoms include:
· Metamorphopsia – straight lines appear wavy
· Blurry or dark spots in the center of vision
· Colors are washed out
· Difficulty recognizing faces and reading
Wet AMD can progress rapidly (days to weeks), so early intervention is essential to maintain and even restore vision. Anti-VEGF drugs can stabilize/improve vision.
Current Treatments
The current treatment market is dominated by anti-VEGF therapies – namely Eylea, Vabysmo, and Lucentis. These treatments are incredibly effective and come as close as possible to curing the disease. The difficulty in this current SoC is that these drugs require frequent intraocular injections (as you can imagine, very unpleasant), monthly or bimonthly. Unsurprisingly, there is significant nonadherence to this frequent injection schedule, which is where Ocular and Eyepoint come into play. As all of the anti-VEGF therapies are essentially curative, the data are virtually identical among all of the options. Below is the data from the Eylea (aflibercept) label.

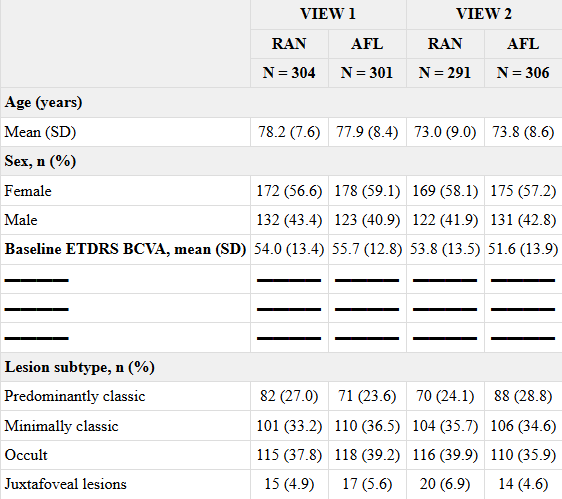
Source: Aflibercept label
Ocular Therapeutix and Axitinib
Ocular Therapeutix is developing a microscopic axitinib (tyrosine kinase inhibitor) implant for the eye to reduce or eliminate the need for ongoing anti-VEGF therapy. It is running a superiority study, termed SOL-1, comparing the efficacy of the implant to no treatment over 9 months, with a 2-dose aflibercept run-in period. The graphic below does a better job of detailing the study design than my description:
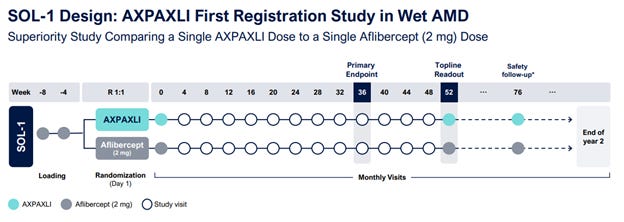
Source: Ocular’s Investor Presentation
This is an ethically questionable and rather unique study design, as it forces the placebo group to receive care below the standard of care. In my opinion, it does not establish superiority to SoC prescribed aflibercept injections. Still, the FDA gave it the green light as a superiority study, so I won’t question it further.
The inclusion criteria are also different. The screened patients must be treatment naïve for wAMD, have a CSFT < 500 um, and a BVCA (best-corrected visual acuity) score of > 54 (20/80). These patients then receive two 2mg aflibercept injections at weeks -8 and -4. Patients who show an increase of 10 BVCA letters and have CSFT of < 250 um or 20/20 vision are randomized 1:1 to the study to receive either the implant or a single dose of aflibercept at the start of the study. The primary endpoint of the study is the proportion of patients who did not lose 15 BVCA letters and did not receive a rescue aflibercept injection. The trial continues through week 52, when the topline readout occurs.
To give a bit of background on axitinib, oral axitinib is dosed at 5mg twice daily for advanced renal cell carcinoma after failure of one systemic therapy. At these doses, it is a rather nasty drug that carries a plethora of adverse effects seen in the tyrosine kinase inhibitor/systemic anti-VEGF class. However, the eye implant carries a cumulative dose of 450 micrograms (the previous version carried 600 micrograms) that slowly elutes over 6-9 months. At these doses, there is really no risk of systemic AEs, even if the entire implant were to enter the bloodstream. Plasma axitinib levels were below the limit of detection in earlier Ocular studies.
The implant showed data consistent with the efficacy observed in earlier studies.
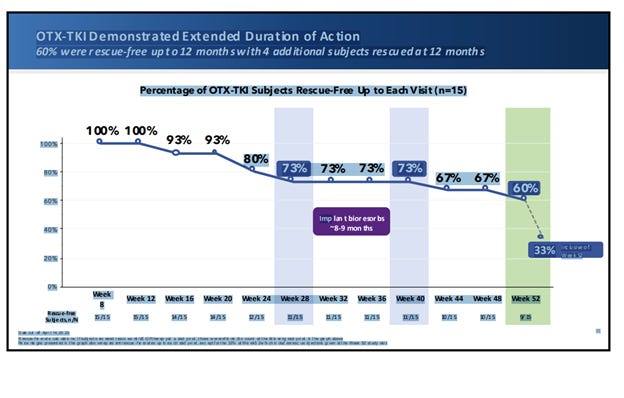
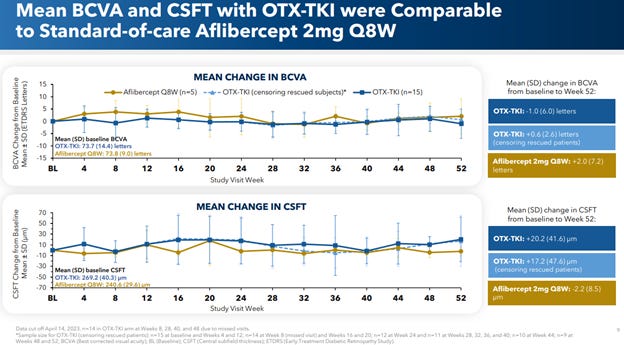
Source: Ocular nAMD Phase 1 Results - https://investors.ocutx.com/static-files/a6148d04-e289-40c0-9b2b-233c22ec0458
An aflibercept injection was also given at the start of the study to both groups. The rescue criteria for this phase 1 study were a loss of 10 BVCA letters or a 75 um CSFT increase and a 5-letter BVCA loss. Importantly, it was noted that the majority of rescues were investigator-initiated rather than being initiated by the rescue criteria.
Ocular Therapeutix slightly modified the formulation based on these phase 1 results to improve drug elution while decreasing the total drug amount in the implant from 0.6mg to 0.45mg.

Source: Patent - https://patents.google.com/patent/WO2024215649A1/en
Given the 73% rescue-free rate from phase 1, combined with the fact that the drug now elutes better, the rescue criteria are more relaxed, and >95% of rescues are per the defined rescue criteria, I expect the rescue-free rate for the Sol-1 phase 3 trial to be around 85+%. Most KOLs would call this a significant win and potentially paradigm-changing for ophthalmology.
However, I have some concerns about how robust the placebo response will be. At first glance, many would assume that the placebo group will face significant vision decline in the absence of treatment over 9 months. Compared to the standard of care, which is an injection either monthly or bimonthly, this treatment regimen is essentially forcing patients off their medication. However, there are some important points to consider. First, at baseline, about 47% of patients lose greater than 15 BVCA letters at 9 months.

Source: Verteporfin label
However, the three lead-in aflibercept injections are likely to last about 3 months before revascularization occurs.

Source: https://www.ophthalmologyretina.org/article/S2468-6530(21)00099-3/fulltext
Therefore, a more accurate representation of the potential placebo response is the proportion who lost >15 letters at 6 months rather than at 9 months, which would put the rescue-free rate at about 65%. However, it is possible, albeit unlikely, that only a subset of patients who revascularize lose 15 letters. If you follow this line of thinking, the placebo-free rate at 9 months could be upwards of 75%.
There are multiple reasons to think this is unlikely to occur, however. First, patients with high baseline visual acuity tend to decline much more than those with lower baseline visual acuity. As you can recall from the inclusion criteria, the patients randomized into the trial have good visual acuity.
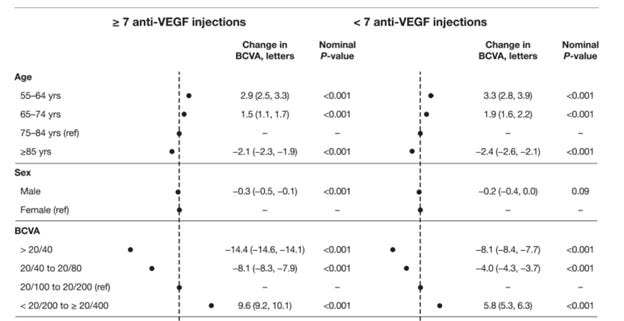
Source: https://www.sciencedirect.com/science/article/pii/S2468653025003100
Second, there may be a reason to think that a few of the patients gained 10 letters from their original baseline and got a bit lucky at randomization. The true gain may be more like 6-7 letters, and the 10-letter may revert to 6-7 letters on the next measurement. Additionally, management has said they are seeing rescues in the blinded data.
Taken together, and to be conservative, I predict the placebo group will be around 65% rescue-free at 9 months, which is enough to achieve the 15% delta needed for statistical significance. Other smart folks have predicted a 50-60% rescue free rate for placebo based on randomized withdrawal simulations.
Lastly, there are some commercial concerns. Ophthalmologists make a ton of money from consistent anti-VEGF injections and may be reluctant to switch to 6-month implants due to the loss of potential revenue. On the other hand, payers will likely save a ton of money over time, so if these implants prove successful in p3 studies, they will push for them to become first-line. Patients, obviously, the most important factor, will also push for less frequent eye injections.